Episode 53: CRP – An important part of a Comprehensive Risk Profile or a Completely Ridiculous Practice- Part II
Episode 53 continues where we left with the whole CRP measurement or no measurement discussion. James and Mike start with the Reynolds Risk Score and show how even at the extremes of CRP, absolute risks only change by around +/- 2% or so. Far more interesting is that there are now 2 studies showing clearly that good estimates of cardiovascular risk can be made without knowing lab values like cholesterol and CRP. All you have to basically do is look at the patient. Mike looks at James and declares that James is at very high risk of annoying Mike – so he does, just to show the evidence is solid.
Show Notes
1) Reynolds Risk Score
2) CRP goes up as weight goes up
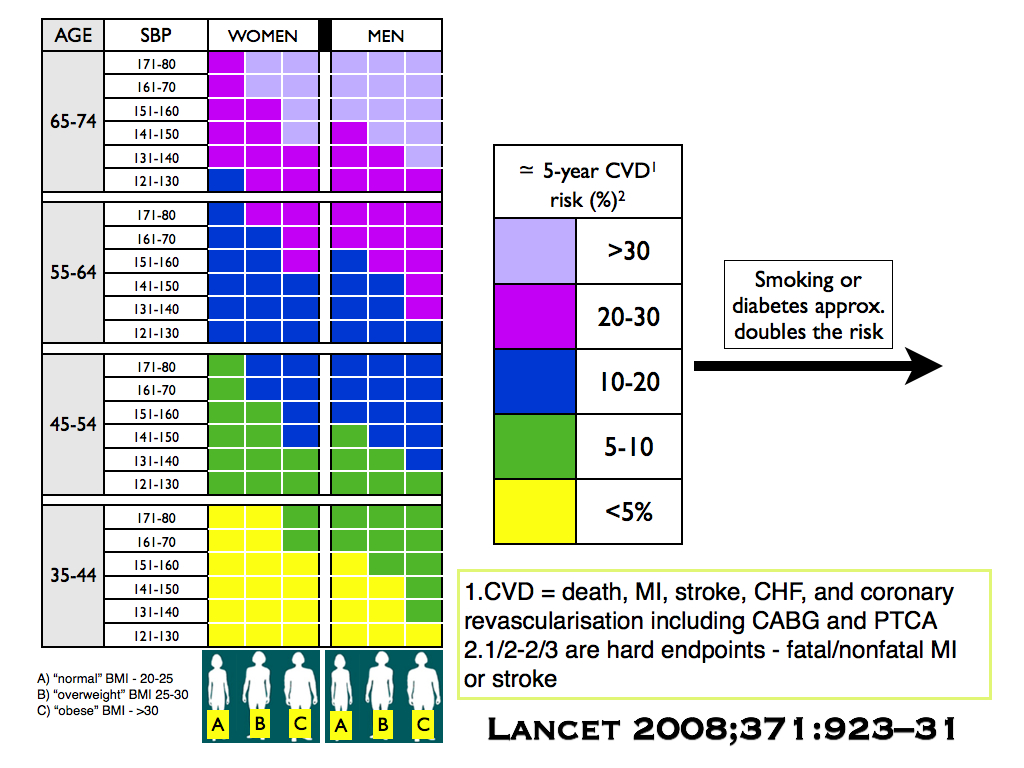
3) Estimating cardiovascular risk estimates without knowing cholesterol or CRP