Episode 52 goes back in time to look in more detail at what we talked about in episode 30; the whole issue of CRP measurement. Mike and James start at the “large” issue of intra-subject variability, then focus on the “small” impact CRP has on absolute risk assessment, and briefly discuss how “accurate” risk assessments are in the first place. Finally they come to the conclusion that, as with most of the podcasts, they are very accurately vague and there is huge intra-podcaster variability.
Show Notes
1) Issues of intra-subject CRP measurement variability
Clinical Chemistry 2001;47:444–50
2) Need for repeat and multiple values
Clinical Chemistry 1997;43:52–8
Ann Clin Biochem 2002;39:85-8
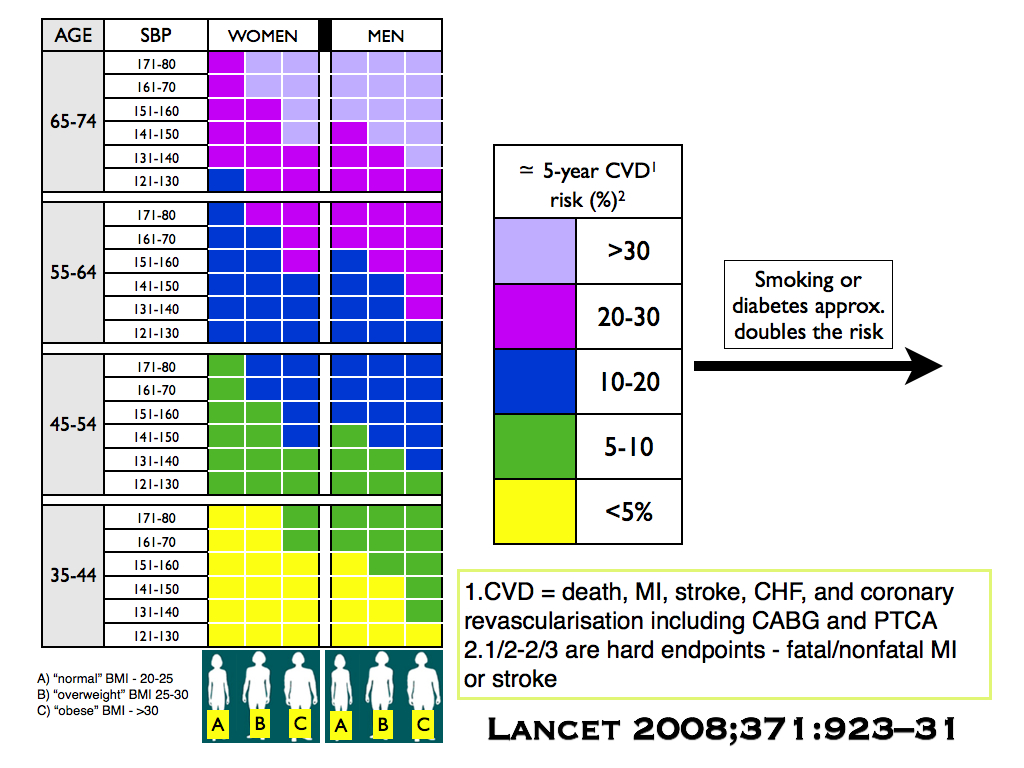
3) Impact on risk assessment of adding CRP to other risk factors
“Our findings suggest that routine measurement of these novel markers [CRP] is not warranted for risk assessment”
Arch Intern Med 2006;166:1368-73
“the addition of multimarker scores [CRP] to conventional risk factors resulted in only small increases in the ability to classify risk”
NEJM 2006;355;2631-9
“CRP does not perform better than the Framingham risk equation for discrimination. The improvement in risk stratification or reclassification …is small and inconsistent”
Int J Epidem 2009;38:217–31
4) Reclassification in risk level when using CRP
Women
Ann Int Med 2006;145:21-9
Men
Circulation 2008;118:2243-51
Net reclassification less than that seen in the above studies
Circ Cardiovasc Qual Outcomes 2008;1:92-7
5) Issue of confidence intervals around risk assessments
J Cardiovasc Risk 2002;9:183-90